What Is Direct Contracting?
A trend our team at Amera is observing this year is health plans searching beyond traditional networks for ways to reduce healthcare costs. We pay close attention to these strategies because TPAs use our technology to process and normalize the irregular claims that cost containment arrangements tend to generate. One strategy gaining momentum is direct contracting.
"Direct contracting" means different things depending on your point-of-view.
For a broker, it may mean adding a Direct Primary Care (DPC) partner or surgical bundle vendor. For a plan administrator, it may mean supporting custom provider contracts, eligibility rules, claims routing, payment logic, and reporting. For a stop-loss carrier, it may mean asking whether a plan has strategies to manage large-claim exposure. For an employer, it may mean giving employees better options without making the plan harder to use.
Historically, direct contracting in the self-funded market was associated with direct primary care. Today, the ecosystem is much larger. Employers are building direct contracting strategies across imaging, surgery, musculoskeletal care, oncology, kidney care, women's health, behavioral health, chronic condition management, and Centers of Excellence.
At its core, direct contracting means a health plan establishes a direct relationship with a provider or specialty vendor rather than relying exclusively on traditional network arrangements.
This article walks through how direct contracting works in the self-funded market, what makes it hard to execute, and what separates plans that do it well from those that struggle.
How Direct Contracting Reduces Costs
The clearest advantage of direct contracting is removing layers that add friction and cost without adding value. Rather than paying rates negotiated through multiple layers of network infrastructure, plans negotiate directly with providers. Transparent pricing is established for specific services.
The categories where this tends to have the most impact are imaging, outpatient procedures, musculoskeletal, and high-cost specialty care like oncology. On the imaging side specifically, site-of-care matters enormously. The same MRI can cost 5x more depending on where it's performed, and traditional networks are rarely incentivised to steer members toward lower-cost settings.
Direct contracting also tends to reduce variation in how care gets delivered. Providers operating under direct contracts often see fewer complications and less unnecessary utilization, which has a compounding effect on total cost of care for conditions like surgery and oncology.
Why Direct Contracting Is Hard to Operationalize
Direct contracting sounds straightforward, but most employers, consultants, and TPAs agree that operationalizing direct contracts is no walk in the park.
The challenge is that direct contracting introduces new workflows into a system that was designed around standard network relationships and claims processing. Every arrangement comes with its own eligibility rules, provider rosters, reimbursement terms, reporting requirements, and member experience considerations.
What looks like a simple provider agreement on paper often requires coordination across navigation teams, claims administrators, providers, and specialty vendors. Members need to know when a program applies and how to access it. Administrators need to identify the arrangement when claims arrive and ensure the correct payment logic is applied. Employers need visibility into utilization, savings, and outcomes.
As more plans adopt specialty carve-outs, Centers of Excellence, bundled payments, and other direct contracting models, the operational complexity grows.
Challenge #1: Navigation Has to Happen Early
Navigation is the muscle holding up the bones of a good direct contract. The best contracts are invisible without a great navigator." Lyn Carter, VP at Health Admins
The biggest opportunity for savings often exists before care is delivered. Once a surgery has been scheduled or a specialist relationship is established, the ability to influence the care journey becomes significantly more limited.
“Few redirections away from non-contracted facilities and surgeons are successful even if the patient's out of pocket is entirely waived.” Keith Smith, Cofounder of the Surgery Center of Oklahoma
Successful direct contracting programs identify opportunities early and engage members before key care decisions are made. Depending on the program, this may involve appointment data, referral activity, prior authorization requests, care navigation workflows, or other signals that indicate a member is entering a high-cost episode of care.
Members can then be guided toward contracted providers through navigation programs, referral workflows, prior authorization processes, advocacy teams, or digital engagement tools.
Challenge #2: Claims Routing Is Difficult
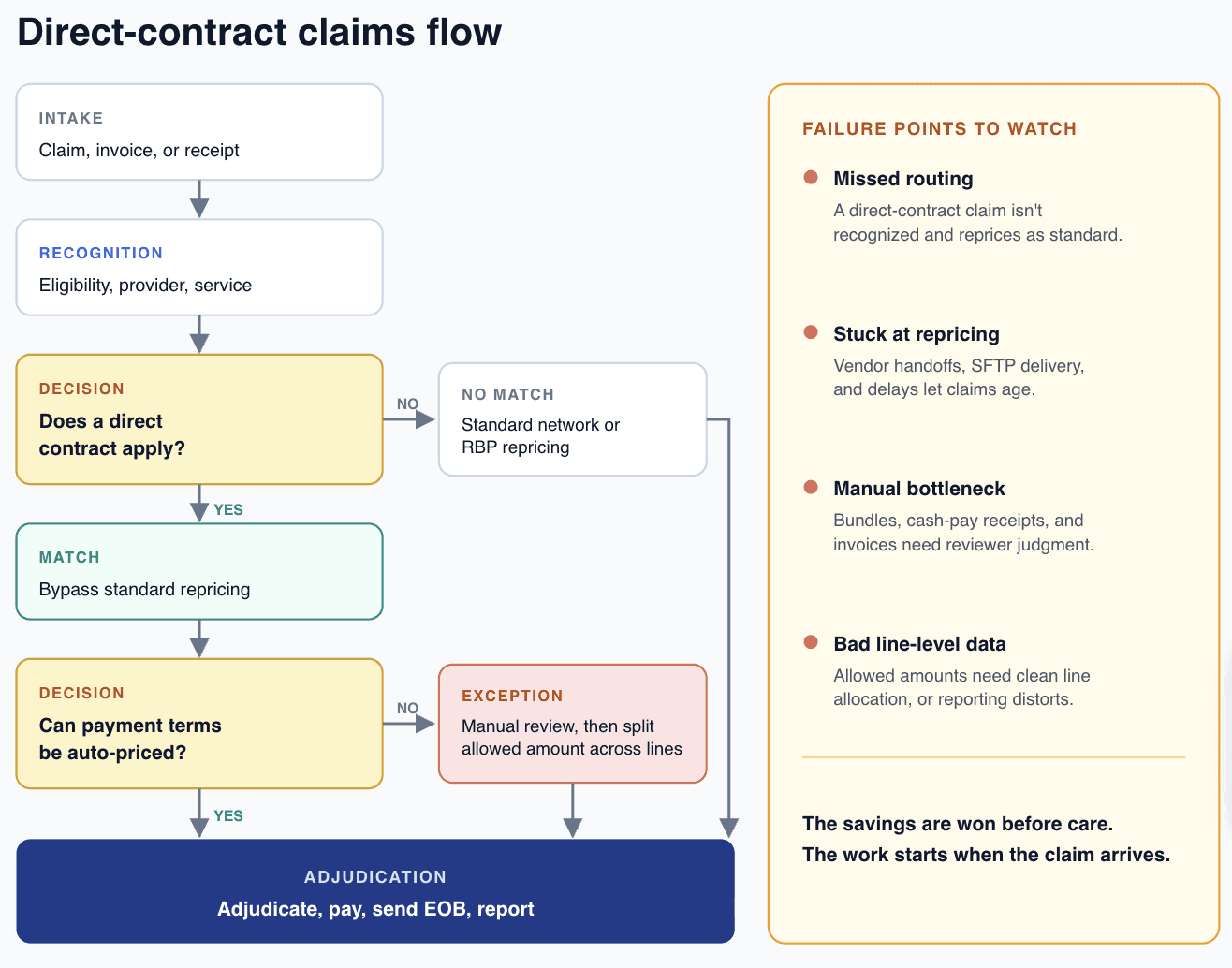
When a claim arrives at the TPA, the routing system has to recognize that a direct contract applies, bypass standard network repricing, and execute a different payment workflow. That logic is typically configured during implementation and can be difficult to test until live claims start hitting adjudication. Problems often surface only after payment issues occur, such as when a provider calls to ask why a claim was processed incorrectly.
The complexity increases with alternative payment models. Cash-pay receipts, invoices, bundled payments, and other non-standard reimbursement arrangements do not arrive through traditional EDI channels and often require additional processing before they can be adjudicated. Service-line carve-outs add another layer of complexity, creating more routing decisions and more opportunities for claims to follow the wrong path.
Challenge #3: It Creates Operational Burden for TPAs
Routing complexity eventually becomes a manual operational burden on TPA employees. When a claim is routed incorrectly, someone has to identify the issue, reconcile the payment, and reprocess the claim.
Non-standard reimbursement models often create manual workflows that sit outside normal claims operations. As the number of direct contracts, carve-outs, and specialty programs grows, so does the volume of exceptions that require human intervention.
The plans that execute direct contracting successfully are usually the ones that invest in the operational infrastructure required to support it. Strong provider data, clear routing rules, automated workflows, and visibility into exceptions help ensure that the administrative complexity does not outweigh the savings opportunity.
What Plans Should Know Before Implementing Direct Contracting
Direct contracting can deliver meaningful savings and clinical value. But to be successful, the following pieces must be in place:
Member Navigation: Members need clear pathways into the program. The best contract delivers little value if members never reach the provider.
Administrative Readiness: Eligibility, provider data, claims workflows, reporting, and payment logic must support the arrangement from day one.
Measurement and Visibility: Plans need a reliable way to understand utilization, savings, outcomes, and operational performance.
The next phase of direct contracting will be defined by making curated care easy to use, easy to administer, and easy to measure.
Direct contracting has evolved from a niche strategy into a major component of self-funded healthcare. The organizations that succeed will be the ones that approach direct contracting as both a care strategy and an operational challenge.
Download the high-resolution PDF of our TPA Ecosystem Map